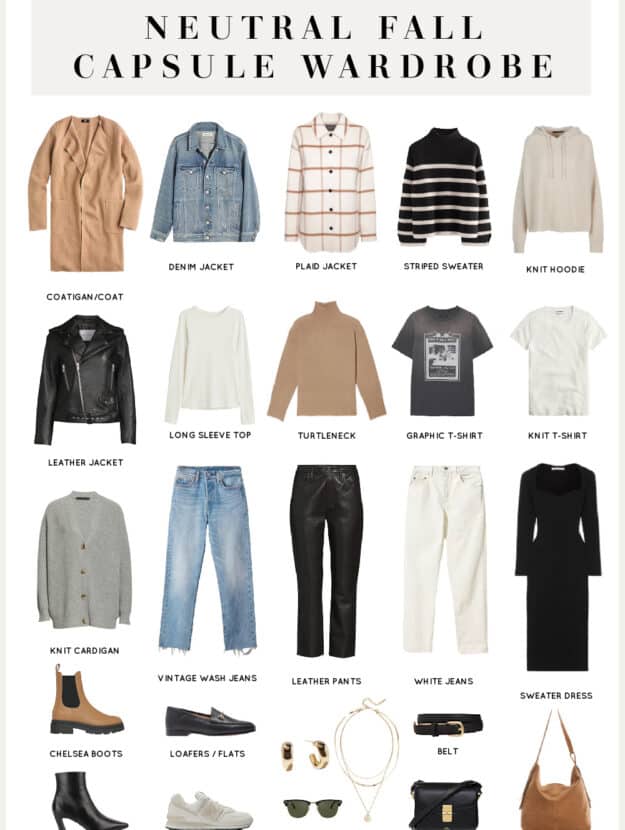
En esta guía te compartimos ideas para que puedas encontrar el look ideal.

Opta por prendas de gran tamaño, como chaquetas y abrigos, que aportan un aire desenfadado y cómodo a cualquier atuendo. Los tonos neutros y los estampados sutiles son ideales para combinar con otras piezas, creando un look equilibrado y moderno.
Incorpora accesorios llamativos, como cinturones anchos y joyas de gran tamaño, que pueden transformar un conjunto sencillo en algo extraordinario. Los bolsos de mano estructurados también están en auge, ofreciendo tanto funcionalidad como estilo.
Los tejidos sostenibles están ganando popularidad, así que considera elegir marcas que priorizan la ética en su producción. Las prendas de algodón orgánico y lino no solo son amigables con el medio ambiente, sino que también ofrecen comodidad y frescura.

Las faldas midi y los pantalones de tiro alto son opciones versátiles que se adaptan a diversas ocasiones. Combínalos con blusas ajustadas o camisetas básicas para un look equilibrado y chic.
Finalmente, no subestimes el poder de los colores vibrantes. Los tonos saturados, como el verde esmeralda y el azul cobalto, están en auge y pueden añadir un toque de energía a tu guardarropa.
Key Trends in Women’s Fashion for 2023
Los trajes de dos piezas son tendencia este año, brindando versatilidad y frescura. Elige tonos suaves para una apariencia sofisticado.
Los diseños florales vuelven con fuerza, notablemente en vestidos. Combina estampados y prendas neutros para un contraste llamativo.
Las texturas ecológicos cobran importancia en la moda, fomentando una sensibilidad ambiental. Investiga etiquetas que utilicen materiales reciclados.
Los complementos de gran tamaño se han convertido en indispensables. Pendientes voluminosos y bolsos espaciosos aportan un matiz atrevido a cualquier atuendo.
| Tendencia | Descripción |
|---|---|
| Conjuntos de dos piezas | Comodidad y elegancia en un solo look. |
| Estampados florales | Regreso de los diseños vibrantes en blusas y vestidos. |
| Tejidos sostenibles | Materiales ecológicos que promueven la conciencia ambiental. |
| Accesorios oversized | Pendientes y bolsos de gran tamaño que destacan. |
Bold Colors: How to Incorporate Vibrant Hues into Your Wardrobe
Para añadir tonos intensos a tu vestuario, considera combinaciones de matices que contrasten. Por ejemplo, una camisa roja puede verse espectacular con jeans azules. No temas a mezclar tonos inesperados, como naranja con turquesa.

Accesorios son una manera fácil de incorporar huesos llamativos. Un bolso de color brillante o calzado en un tono audaz pueden cambiar un outfit sencillo en algo notable.
Las capas también son efectivas para introducir tonos vivos. Un abrigo de tonalidad intensa sobre una camiseta neutra puede crear un aspecto equilibrado y atractivo.
Considera prendas con patrones que contengan colores brillantes. Un vestido con motivos coloridos puede ser el centro de tu atuendo, permitiendo que el resto de la ropa sea más discreta.
Finalmente, recuerda que el maquillaje también puede reflejar tu elección de colores. Un labial intenso puede unir todo el conjunto y añadir un toque de carácter.
Oversized Silhouettes: Styling Tips for Comfort and Chic
Opta por prendas de gran tamaño que se ajusten a tu figura, como blusas sueltas o chaquetas amplias. Estas piezas no solo ofrecen comodidad, sino que también aportan un aire desenfadado a tu atuendo.
Combina una camiseta oversized con unos pantalones ajustados para equilibrar la silueta. Este contraste crea un look armonioso y estilizado.
- Elige tejidos ligeros y transpirables para mantener la frescura.
- Incorpora capas, como un abrigo largo sobre un vestido fluido, para añadir dimensión.
- Utiliza accesorios minimalistas, como collares delicados o pendientes pequeños, para no sobrecargar el conjunto.
Los zapatos son clave; opta por zapatillas deportivas o botines para un toque moderno. Evita los tacones altos, ya que pueden romper la estética relajada.
Experimenta con colores neutros y patrones sutiles. Los tonos tierra o pasteles son ideales para un look equilibrado y sofisticado.
- Prueba con un cinturón para definir la cintura y dar forma a la silueta.
- Combina diferentes texturas, como mezclilla con lana, para un efecto visual interesante.
- Juega con las proporciones; una prenda oversized en la parte superior puede ser complementada con una falda corta o pantalones cortos.
Recuerda que la confianza es clave. Lleva lo que te haga sentir cómoda y segura, y tu atuendo reflejará tu personalidad.
Sustainable Fashion: Choosing Eco-Friendly Brands
Opta por marcas que utilizan materiales orgánicos y reciclados, como Patagonia y Eileen Fisher. Estas empresas se comprometen a reducir su huella ambiental mediante prácticas responsables.
Investiga sobre la transparencia de las marcas. Busca aquellas que proporcionan información clara sobre su cadena de suministro y procesos de producción, como Reformation y Everlane.
Considera la durabilidad de las prendas. Elige ropa de alta calidad que resista el paso del tiempo, evitando así el consumo excesivo. Marcas como People Tree ofrecen opciones sostenibles y duraderas.
![]()
Apoya a diseñadores locales que utilizan técnicas artesanales y materiales sostenibles. Esto no solo promueve la economía local, sino que también reduce el impacto ambiental del transporte.
Explora opciones de segunda mano. Tiendas como ThredUp y Depop permiten encontrar prendas únicas y reducir el desperdicio textil.

Infórmate sobre las certificaciones ecológicas. Busca etiquetas como Global Organic Textile Standard (GOTS) o OEKO-TEX que garantizan prácticas sostenibles en la producción.

Participa en iniciativas de intercambio de ropa. Estas actividades fomentan la reutilización y permiten renovar el guardarropa sin generar nuevos residuos.
Statement Accessories: Elevating Outfits with Unique Pieces
Incorpora pendientes llamativos para transformar un atuendo sencillo en algo extraordinario. Opta por piezas que resalten tu personalidad y agreguen un toque especial.
![]()
- Los collares de declaración pueden convertirse en el punto focal de tu look. Encuentra diseños con formas geométricas que capturen la atención.
- Los pendientes oversized son perfectos para complementar un peinado recogido. Selecciona colores vibrantes o metales brillantes.
- Las pulseras apiladas ofrecen una opción versátil. Mezcla diferentes texturas y estilos para un efecto dinámico.
Considera incorporar un sombrero llamativo o un cartera de diseño único. Estos elementos tienen el potencial de elevar cualquier conjunto básico.
- Escoge un sombrero de ala ancha o un beanie con estampados.
- Opta por un bolso estructurado en un color contrastante.

Recuerda que la clave está en equilibrar las piezas. Evita saturar el atuendo; elige uno o dos accesorios que realmente hablen por sí mismos.
Layering Techniques: Mastering the Art of Fashion Layers
Para lograr un look sofisticado, combina textiles finos con capa exterior que añadan profundidad. Opta por camisetas de tonos suaves como base, y añade un cárdigan en la parte superior.
Utiliza bufandas como accesorios para dar textura. Las bufandas largas pueden ser diseñadas de diferentes maneras, creando nudos que aportan carácter.
Incorpora ropa de distintas medidas para jugar con la silueta. A modo de ejemplo, combina una camiseta cropped con jeans de tiro alto para un resultado equilibrado.
Elige texturas contrastantes para diversificar el atuendo. Mezcla seda con denim para construir un outfit atractivo y llamativo.
Finalmente, no olvides las botas. Opta por zapatos de plataforma que sean acordes a la paleta de colores de tu atuendo. La elección del calzado puede alterar completamente la imagen final.
Footwear Trends: What Shoes Are Must-Haves This Season
Las botas de combate son imprescindibles este periodo. Su diseño robusto y versatilidad las convierte orden en casa una opción ideal para cualquier atuendo. Combínalas con pantalones ajustados o faldas midi para un look equilibrado.
Los zapatillas deportivas de estilo retro están en auge. Opta por modelos con colores vibrantes y detalles llamativos. Son perfectas para un look casual y cómodo, ideales para el día a día.

Las sandalias de plataforma regresan con fuerza. Este calzado no solo añade altura, sino que también proporciona comodidad. Úsalas con vestidos fluidos o pantalones cortos para un aire relajado.
Los zapatos de tacón cuadrado son una opción elegante y práctica. Su diseño permite mayor estabilidad, lo que los hace perfectos para ocasiones formales. Combínalos con trajes sastre o vestidos ajustados.
Las botas de vaquero están de vuelta. Este calzado aporta un toque bohemio a cualquier conjunto. Úsalas con jeans de tiro alto o falda larga para un look desenfadado.